Case history
December 21,2021
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/ guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This e- log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
Date of administration:18-12-2021
A 60 year old male patient came to the opd with chief complaints of fever since 5 days , constipation & short ness of breathe since 4 days, burning micturation since 10 days, cough since 6 days.
History of present illness :
Patient was apparently asymptomatic 10 days back then he complaint of high grade fever associated with nausea , no rigor & chills, dry cough, decreased urine out put with burning micturation ,constipation , short ness of breathe
He went to local doctor & was diagnosed as kidney injury
Past history:
Known case of diabetes & hypertension since 30 years
Not a know case of asthma, epilepsy, TB
Personal history:
Dite : mixed
Appetite : normal
Sleep : adequate
Bowel & bladder movements : decreased
Occasionally alcoholic
Family history:
No similar complaints in the family
General physical examination:
Patient is conscious, coherent, co-operative
He is well oriented to time place and person
He is moderately build & nourished
No icterus, cyanosis, clubbing, generalized lymphadenopathy , pedal edema



Vitals :
Temperature:101F
BP :120/70mmHg
PR:80bpm
Respiration rate: 19cpm
Systemic examination :
Cardiovascular system :
S1 and S2 heard
No murmurs
Respiratory system :
Normal vesicular breath sounds are heard
Position of trachea : central
BAE +
Per abdomen :
Soft & distended
Guarding positive
CNS :
No abnormality directed
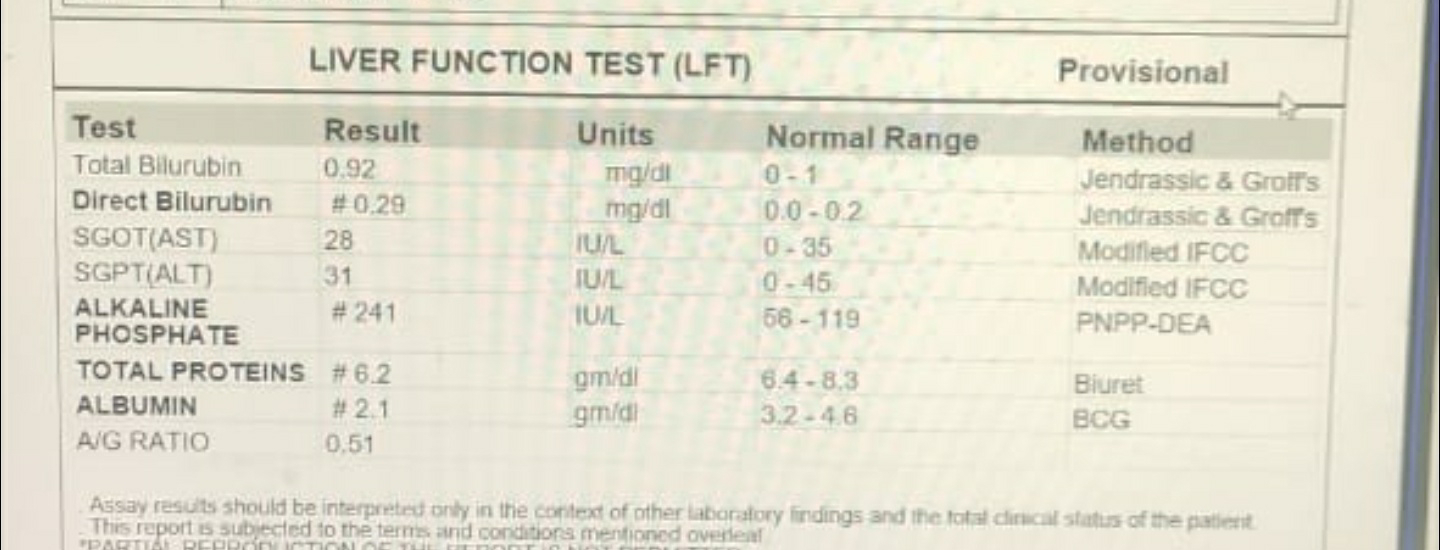
Investigations










KCl 1 ampoule in 10 ml NS over 4 hrs.
Inj. PANTOP 40 mg IV OD
Inj. MONOCEF 1 gm IV BD
Inj. ZOFER 4 mg IV SOS
Inj. NEOMOL 1gm IV SOS
Tab. DOLO 650 mg PO TID
Tab. AMLONG 2.5 mg PO OD
Inj. HUMAN ACTRAPID SC Acc to GRBS
Syp. LACTULOSE 10 ml PO BD



Comments
Post a Comment